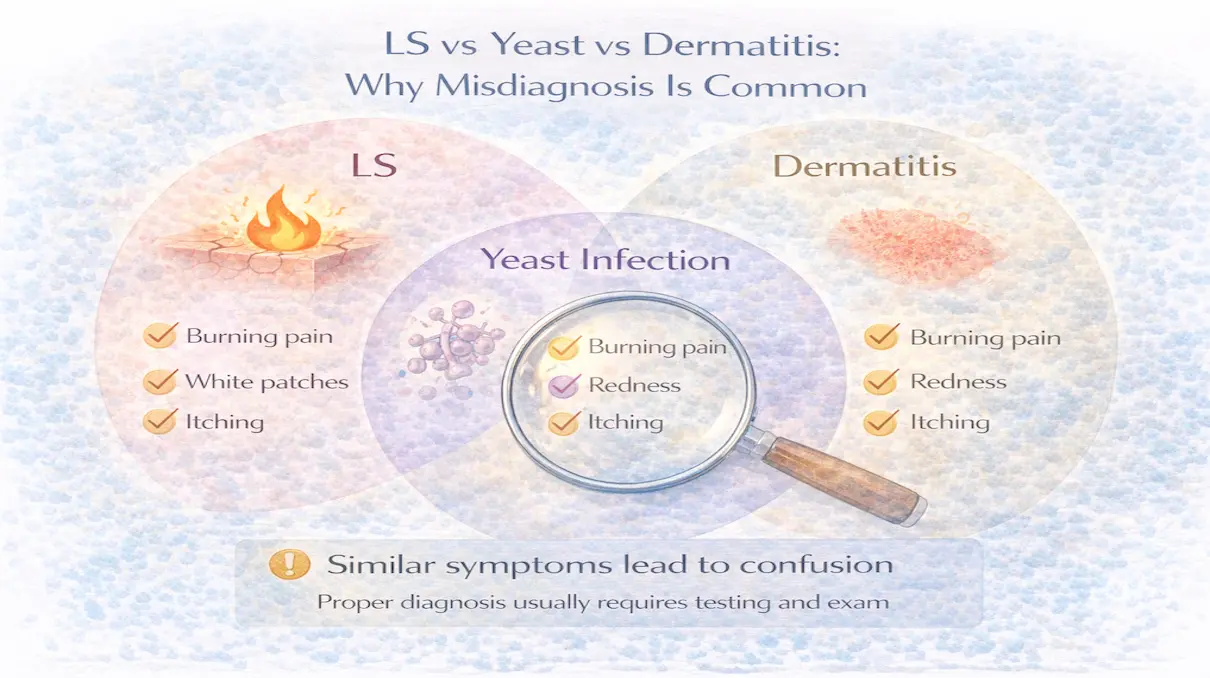
LS vs Yeast vs Dermatitis: Why Misdiagnosis Is Common
Many people with lichen sclerosus spend months, sometimes years being treated for the wrong condition.
They’re told it’s yeast.
Then contact dermatitis.
Then irritation.
Sometimes all three.
Treatments change, symptoms fluctuate, and nothing fully stabilizes.
This is not because LS is rare, it’s because LS often looks and feels like other conditions, especially early on.
Understanding how LS differs from yeast infections and dermatitis explains why misdiagnosis is so common and why symptoms often persist despite “treatment.”
Why These Conditions Are Confused
LS, yeast infections, and dermatitis all affect sensitive genital skin.
They can all cause:
- burning
- itching
- soreness
- redness
- discomfort with movement or sex
But the mechanism underneath is completely different, and that determines which treatment works.
How Yeast Infections Behave
Yeast infections are caused by fungal overgrowth.
Typical features include:
- itching as the dominant symptom
- redness and irritation that fluctuate quickly
- discharge (in women)
- rapid response to antifungals
When yeast is treated correctly, symptoms usually improve within days.
If antifungal treatment does nothing, or symptoms return immediately, yeast is unlikely to be the primary problem.
How Contact or Irritant Dermatitis Behaves
Dermatitis is a reaction to something external:
- soaps
- wipes
- detergents
- pads
- friction or moisture
Symptoms usually:
- correlate with exposure
- improve when the trigger is removed
- respond to short courses of mild anti inflammatory treatment
Dermatitis tends to resolve fully once the irritant is eliminated.
Persistent symptoms despite trigger avoidance suggest something else is going on.
How Lichen Sclerosus Behaves Differently
LS is a chronic inflammatory skin condition, not an infection and not a simple reaction.
Key features include:
- symptoms that wax and wane over time
- burning or tightness more than itching
- sensitivity without obvious redness
- symptoms that improve with steroids and return when stopped
- gradual skin changes over months or years
Unlike yeast or dermatitis, LS does not resolve on its own.
Why Antifungals Often “Almost Help”
Many people report partial improvement with antifungals.
This happens because:
- antifungal creams are occlusive
- they reduce friction
- they temporarily soothe nerves
This can mask LS symptoms without treating inflammation.
When symptoms return, stronger antifungals are often prescribed — delaying the correct diagnosis.
Why Steroids Confuse the Picture
Steroids suppress inflammation, so they help both dermatitis and LS.
This is why:
- short steroid courses may improve symptoms
- symptoms return when steroids stop
The difference is duration and pattern.
Dermatitis resolves completely.
LS improves but requires ongoing management.
Importantly, not all LS needs the same steroid strength.
- Clobetasol is appropriate for strong, active inflammation
- Mometasone is often enough for moderate inflammation
- Hydrocortisone can be sufficient for mild inflammation or tapering
Failure to respond to mild steroids does not rule out LS, it often means inflammation is stronger.
Why LS Is Often Missed Early
Early LS may not show classic signs.
Skin can look:
- slightly pale
- slightly shiny
- or completely normal
Symptoms may be intermittent.
Without obvious changes, LS is often labeled as “recurrent yeast” or “chronic irritation.”
This delays appropriate treatment.
Why Misdiagnosis Matters
Delayed diagnosis leads to:
- prolonged uncontrolled inflammation
- unnecessary antifungal use
- repeated flares
- increased risk of structural changes
Early control dramatically improves long term outcomes.
When to Re Evaluate the Diagnosis
LS should be considered when:
- symptoms persist despite antifungals
- symptoms recur repeatedly without clear triggers
- steroids help but symptoms return when stopped
- burning or tightness dominates over itching
Biopsy may be helpful, but clinical patterns matter just as much.
Final Thought
Yeast infections and dermatitis are common, but they are not chronic inflammatory diseases.
When symptoms persist, fluctuate, and partially respond to steroids, LS must be considered.
Correct diagnosis allows:
- appropriate steroid potency selection
- proper tapering
- barrier protection
- long-term stability
And prevents years of unnecessary frustration.